Procedures
Pacer/Defibrillator (AICD) Implantation
Dr. Marieb has been implanting these devices for over 25 years. Pacemakers are typically implanted for slow heartbeats. Defibrillators are recommended for patients who have had malignant ventricular arrhythmias such as ventricular tachycardia or ventricular fibrillation causing sudden cardiac death or patients at risk for these events. The defibrillator shocks the heart out of these life threatening arrhythmias. These devices typically take an hour to an hour and a half to implant. Patients are generally kept in the hospital overnight but in some instances can even be sent home on the same day. These devices are placed transvenously with wires running into the heart. In general these devices do not limit a patient's activities or the lifestyle. In fact the newer generations of these devices are even compatible with MRI scanning. These devices can now be followed remotely from home, with data transmitted to the physician’s office. Please also look on this site for variations including subcutaneous defibrillators, HIS Bundle Pacing, cardiac resynchronization therapy, as well as remote monitoring of implantable devices. See below for a video on the defibrillator implant procedure. A pacer implant is performed in the same way.
Cardiac resynchronization (biventricular pacing) therapy
This technology is used in patients who have a delay in electrical activation from the right to left ventricle. This delay (“dyssynchrony”) can be caused by pacing the right ventricle or by left bundle branch block branch block, and results in weakening of the heart and congestive heart failure (CHF).
This situation is corrected by implanting a pacing lead into the coronary sinus, a vein that runs over the outer surface of the left ventricle. Now, the left and right ventricles can be paced simultaneously, “resynchronizing” the contraction between the right and left sides of the heart. This can lead to a significant improvement in heart function, reducing the symptoms of congestive heart failure, and often significantly improving quality of life.
Cardiac resynchronization can be undertaken as part of a pacemaker implantation procedure, and can be combined with defibrillator (AICD) implantation.

Quadrapolar lead technology where pacing the left ventricle can be undertaken from 4 different electrodes has improved the success rate of the procedure.

Subcutaneous (SQ) AICD implantation
This automatic implantable defibrillator, recently approved to treat sudden cardiac death, marketed by Boston Scientific Corporation.. Conventional implanted defibrillators require leads be placed through veins and placed directly into the heart. This novel device avoids placing any leads into the heart. Placing leads through blood vessels to the inside of the heart can cause acute problems during the implant of a defibrillator, including cardiac perforation or a collapsed lung. In the longer term, endocardial leads have been shown, especially over time, to ultimately fail to function. They can also cause vessel obstruction, valve malfunction, or become infected. This newer device avoids these complications.
The lead used with this device runs subcutaneously, under the skin over the front of the chest; again, there is no "hardware" placed in the blood vessels or heart. The shock waveform is delivered between the lead and the device itself.


The above two photos are of the SQ AICD. Notice that there is no lead in the heart or blood vessels

The above photo is of a conventional AICD, where there is lead in both the heart and blood vessels.
The SQ AICD is not indicated for those who need pacing for bradycardia or cardiac resychronization.
This device may be ideal for young patients especially, so they can avoid the long term problems associated with endocardial/endovascular leads.
Micra™ (leadless pacemaker) implantation
This miniature pacemaker, manufactured by Medtronic, is implanted directly into the heart, thereby avoiding pacemaker leads (wires) and avoiding the surgical creation of a pacemaker pocket. The device is implanted via the femoral vein. Not having pacemaker leads reduces the risk of lead issues, including degeneration, fractures, and insulation issues.
For a video of the implantation procedure, see the link below:

FAQ
Is Micra the right pacemaker for all patients?
No. Micra is intended for patients who need a single chamber pacemaker (also known as a ventricular pacemaker, or VVIR). Talk to your doctor about the suitability, benefits, and risks of Micra for you.
How is Micra placed into my heart?
Your doctor will insert a "straw-like" catheter into a vein in your upper thigh and use the catheter to move Micra into the right ventricle of your heart. The catheter is then removed.
Are MRI scans okay with my Micra?
Micra was designed, tested, and approved to be used safely with MRI scanners. You can undergo an MRI scan as long as patient eligibility requirements are met. Your pacemaker ID card specifies the implanted device model. If your doctor has questions about scanning eligibility, he or she should contact a Medtronic representative or Medtronic Technical Services.
Will items containing magnets affect my Micra?
Maybe. We recommend keeping items containing magnets at least 6 inches away from an implanted pacemaker. This includes mobile phones, magnetic therapy products, stereo speakers, and handheld massagers. We do not recommend putting a mobile phone in your shirt pocket or using magnetic mattress pads and pillows.
Is it safe to go through an airport metal detector?
Yes, you can safely go through airport security with this device.
Are household appliances safe to use?
Yes, household appliances that are properly maintained and in good working order are safe. This includes microwave ovens, major appliances, electric blankets, and heating pads.
Can I exercise, resume my regular activities?
Yes, you should be able to return to your usual activities, as long you do not exceed your fitness level. Discuss questions about specific activities with your doctor.
Does Micra last forever?
No, Micra has a battery and the battery life depends on your heart condition. The estimated average longevity is 12 years.3 Individual patient experience may vary. Your doctor will check on the battery when you come in for a checkup.
What happens when the Micra battery runs low?
Micra is designed to provide options when a new device is needed. It may be turned off and a new Micra or a traditional system may be implanted. The Micra also offers a retrieval feature to enable retrieval, when possible. Your doctor will determine what is best for you.
How often will I need to visit the doctor after Micra is implanted?
Your doctor will decide how often he or she wants to see you. Typically, your first follow-up appointment is one month after implant, with additional follow-ups every 6-12 months.
Linq™ implantable cardiac monitor
This miniature implantable cardiac rhythm monitoring device can be implanted under the skin within a few minutes under local anesthesia. The Reveal Linq Insertable Cardiac Monitor (ICM) Marketed by Medtronic Inc. is the smallest implantable cardiac monitor available to patients.
The Reveal Linq ICM is approximately one-third the size of a AAA battery (~1 cc), making it more than 80 percent smaller than other ICMs. The device is part of a system that allows physicians to continuously and wirelessly monitor a patient’s heart for up to three years, with 20 percent more data memory than its larger predecessor, the Reveal XT.
The system provides remote monitoring through the CarelinkNetwork in which physicians can request notifications to alert them if their patients have cardiac events. The Reveal Linq ICM is indicated for patients who experience symptoms such as dizziness, palpitation, syncope and chest pain that may suggest a cardiac arrhythmia, and for patients at increased risk for cardiac arrhythmias.
Placed just beneath the skin through a small incision of less than 1 cm in the upper left side of the chest, the Reveal Linq ICM is often nearly invisible to the naked eye once inserted. The device is placed using a minimally invasive insertion procedure, which simplifies the experience for both physicians and their patients. The Reveal Linq ICM is MR-Conditional, allowing patients to undergo magnetic resonance imaging (MRI) if needed.
The Reveal Linq system also includes the new MyCareLink Patient Monitor. That is a simplified remote monitoring system with global cellular technology that transmits patients’ cardiac device diagnostic data to their clinicians from nearly any location in the world.

Atrial fibrillation ablation
Atrial fibrillation ablation is a highly complicated and technically challenging procedure. Common to all of these procedures is electrical isolation of the pulmonary veins, which are common sources of atrial fibrillation. However in many cases additional areas undergo ablation. The procedure is generally performed under general anesthesia, and takes many hours, especially in more resistant cases. The procedure involves the insertion of multiple catheters into the femoral veins. Intracardiac echocardiography and an electro-anatomical mapping system are used to aid in the procedure.
Please see other related technologies and procedures included on this website including balloon cryoablation, FIRM Rotor mapping and ablation, Hybrid Procedures, contact force sensing technology, and Esosure esophageal stylet. All of these are relevant to atrial fibrillation ablation.

Atrial Fibrillation (AF) Ablation Frequently Asked Questions (FAQ’s)
How long does the procedure take?
The procedure takes many hours, especially in patients who are in persistent atrial fibrillation. A bulk of the time is taken in setting up the patient, placing them under general anesthesia, inserting catheters, creating a geometry of the heart, mapping the signals, and eventually performing the ablation. Procedures can take up to 8 hours.
What type of anesthesia is used?
Typically general anesthesia is used.
How long am I kept in the hospital after the procedure?
Most patients are discharged on the following day, although if there are additional issues occurring after the ablation patients can be kept for few days in the hospital.
How will I feel after the procedure?
This varies. Some patients feel fairly well the following day. However many patients feel as if they were "hit by a truck". Patients are often fatigued and can have some chest discomfort. We recommend taking an average of one week off from work although this will vary.
Why are blood thinners continued throughout the procedure?
This is been shown to be the safest way to do the procedure. Although bleeding may be more likely the chance of a stroke is reduced.
What additional medications will be given to me before and after the procedure?
Starting prior to the procedure two medications will be given to you to help protect your esophagus. After the procedure you will typically be placed on two separate diuretics. Patients typically will accumulate fluid as a result of the procedure and usually for a week after the procedure the diuretics are given. Sometimes anti-arrhythmic medications are given for sometime after the procedure to prevent early recurrences of the arrhythmia. Also, if AF does occur after the procedure, anti-arrhythmic medications may also be prescribed, and often may be more effective than prior to ablation.
Why is an MRI or CT scan done prior to the procedure?
This pre-procedure imaging helps with defining your atrial and pulmonary vein anatomy and the images are used during the procedure to help guide the location of the ablation.
What is the success rate of the procedure?
This depends on many factors. It is very important to note that atrial fibrillation ablation is not a perfect procedure. There can be many areas in both atria that can serve as drivers for atrial fibrillation, and it can be difficult to identify and successfully ablate all of these areas in a single procedure. In addition, other areas can develop over time, so that a procedure can be successful for some time then stop working. The highest success rate is in patients who have recent onset of their arrhythmia, have paroxysmal atrial fibrillation (meaning the AF lasts for shorter periods and stops on its own), have normal or only slight atrial enlargement, are not overweight, do not have sleep apnea, and whose blood pressure is well controlled. In this group of patients the success rate for a single procedure can be as high as 75-80 percent. In most of these patients, the drivers for atrial fibrillation are in the pulmonary veins, and can be cured by conventional pulmonary vein isolation. In patients with longer duration of atrial fibrillation, persistent AF (meaning in it continuously or requiring cardioversion), who have significant atrial enlargement, who are overweight, who have sleep apnea, or who have poorly controlled hypertension or continued alcohol use, the success rate can be lower, even as low as 50% long term. We therefore recommend before an ablation aggressive weight loss, evaluation and treatment of sleep apnea, aggressive control of blood pressure to completely normal values, and minimizing alcohol intake.
Does AF occurring in the first month or two after ablation mean that the procedure did not work?
No. Although we would rather not see arrhythmias during this time (the time period after ablation is often referred to in studies as the “blanking period”), sometimes these arrhythmias quiet down on their own. The thought is that the ablation can cause some irritation that eventually quiets down. However, the procedure can be unsuccessful in a significant portion of patients, and additional procedures may be necessary (see below).
Will more than one procedure be required to satisfactorily treat my atrial fibrillation?
As noted above, atrial fibrillation ablation is not a perfect procedure and the success rates are unfortunately lower than we would like, especially in patients with persistent atrial fibrillation with enlarged atria. Therefore, a significant proportion of patients undergoing atrial fibrillation ablation will require repeat procedures. We have seen patients who require three and rarely four procedures to treat their AF. The good news is that often the repeat procedures are shorter in duration and with multiple procedures success rates even in tougher cases can approach 90 percent.
What are the potential complications of atrial fibrillation ablation?
There are many potentially serious complications of this procedure. These include (but are not limited to) cardiac perforation (hole in heart, which could require drainage of blood from around the heart or even surgery), stroke, death, valve damage, narrowing of the pulmonary veins (known as pulmonary vein stenosis), heart block requiring pacemaker implantation, damage to blood vessels in the femoral area, hematoma/bleeding, phrenic nerve paralysis (damage to the nerve that supplies the diaphragm muscle causing breathing difficulties). A rare but often fatal complication is the formation of an atrio-esophageal fistula (a connection between the heart and esophagus), which typically forms one to 6 weeks after the procedure; for this reason we ask that you call our office immediately if after ablation you have fever, difficulty swallowing, or neurologic symptoms.
What type of followup is required after the procedure?
Often times an echocardiogram is ordered a week or so after the procedure to rule out any fluid around the heart. Typically you will then be seen in the office a few weeks after the procedure. After that, we may obtain a Holter Monitor, Event Monitor, Alivecor Monitor, or even an Implantable Monitor, to assess the success of the ablation and to pick up any arrhythmias that might not be felt. Subsequently we may see you on an intermittent basis. However we often return the patient back to their primary cardiologist for follow up.
Can I stop my anticoagulant or blood thinner after the procedure?
This is a complex and controversial question. If your risk for a stroke is fairly low (a low CHADSVasc2 score), in many instances with shared decision-making between the doctor and patient going over the risks and benefits of each approach, the anticoagulant may be stopped. In some instances it will be recommended that the anticoagulant be continued indefinitely. In some cases various types of monitoring may help make the decision.
FIRM (Focal Impulse and Rotor Modulation) ablation
This technology uses a multielectrode (64 electrodes) basket recording and mapping catheter to record electrical signals during atrial fibrillation. Areas of rotational (Rotor) and focal electrical activity are identified using specialized computer software and displayed (see videos). These areas are then ablated. Studies have shown that ablation of these areas that may be “drivers” of atrial fibrillation increases the success rate of atrial fibrillation ablation procedures.
This is a computer image of a rotor. This helps guide ablation in this area.
Hybrid atrial fibrillation ablation
The hybrid (also known as convergent) ablation procedure for atrial fibrillation involves both a surgical approach which ablates the outer surface of the heart (and can include ligation/clipping of the left atrial appendage), combined with a subsequent catheter ablation procedure which ablates the endocardial (inner surface) of the heart. The catheter ablation can be performed on the same day of the surgical procedure, on the following day, or at a later date. There are many types of hybrid procedures. For the surgical portion of the procedure, some involve a left-sided thoracoscopic approach, some involve a bilateral thoracoscopic approach, and another involves a sub-xiphoid approach.
Our preferred approach to the hybrid procedure is to have the surgeon perform a left-sided-only thoracoscopic approach where the left atrial appendage is clipped using an Atricure clip, the left-sided pulmonary veins are isolated using a radio frequency clamp, and the posterior wall is ablated.
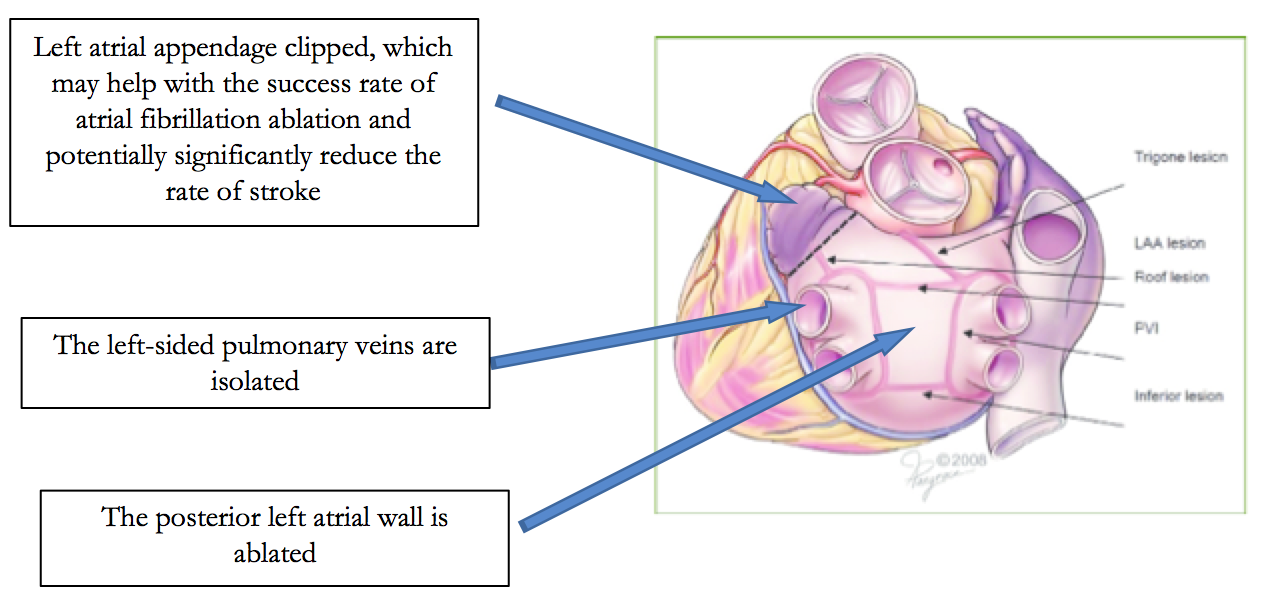
Subsequently, weeks later, catheter ablation is performed to complete the posterior wall ablation, right-sided pulmonary vein ablation, possibly additional ablation in the left atrium, and then right atrial ablation.
The advantage of this procedure is theoretically it may be more effective than catheter ablation alone. This would be especially true for persistent atrial fibrillation. In addition, because the appendage is clipped theoretically this may significantly reduce the chance of stroke and even allow discontinuation of anticoagulation.
Balloon Cryoablation of atrial fibrillation
This new technology uses a balloon catheter, which freezes and thereby ablates the tissue around the pulmonary veins, electrically isolating them. Instead of heating the tissue to destroy it as is the case with radio frequency catheter ablation, this technique uses extremely cold temperatures. A big advantage of this procedure is that it is much faster than ablatingin a point-to-point manner with a radiofrequency ablation catheter. Disadvantages include a higher incidence of phrenic nerve injury, and the fact that it is not as useful for patients with persistent atrial fibrillation, who often require ablation in other areas than the pulmonary veins.
Below is additional information regarding Cryoballoon Ablation from the Medtronic website, manufacturers of the Arctic Front Advance cryoablation catheter.
TREATING PAROXYSMAL ATRIAL FIBRILLATION WITH ARCTIC FRONT ADVANCE CARDIAC CRYOABLATION CATHETER
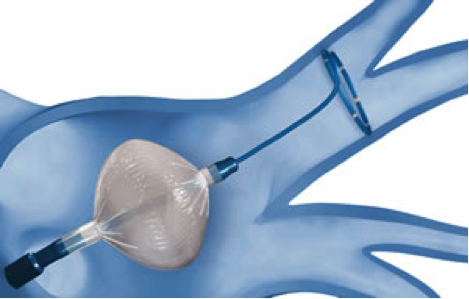
One method for treating paroxysmal atrial fibrillation (PAF) is cryoablation using the Arctic Front Advance™ cryoballoon catheter. As its name indicates, the Arctic Front Advance cryoballoon delivers a refrigerant through an inflatable balloon to freeze tissue and disable unwanted electrical circuits that contribute to PAF.
Arctic Front Advance is a safe, effective, efficient and straightforward medical device for treating PAF. This second generation technology builds upon the proven effectiveness of the original Arctic Front cryoballoon and the two technology platforms have been used to treat over 100,000 patients in more than 800 centers worldwide. Because of its balloon shape, Arctic Front Advance allows physicians to reach and treat pulmonary veins (the site of unwanted electrical currents which trigger your AF) quickly and efficiently. As with any medical procedure, there are benefits and risks with catheter ablation.
Many patients who were treated with Arctic Front Advance cryoballoon experience a welcome improvement in their quality of life as unpleasant symptoms such as shortness of breath, fatigue, and weakness lessen or disappear.

Arctic Front Advance Cryoballoon
ARCTIC FRONT ADVANCE CRYOBALLOON IN ACTION
Cryoablation prevents unwanted electrical currents from traveling from the pulmonary veins (large blood vessels that carry blood from the lungs to the left atrium of the heart) and spreading to the atria (the upper chambers of the heart). This is done with a technique known as pulmonary vein isolation that targets the tissue where the veins and the atria connect and prevents it from spreading unwanted electrical currents. The Arctic Front Advance cryoballoon catheter was developed specifically to achieve pulmonary vein isolation.
In the procedure, the physician makes a small cut in the groin area through which to insert the catheter. The physician threads the catheter to the left atrium of the heart. Then he/she creates a puncture in the wall that separates the left and right sides of the heart. The puncture provides access to the left atrium. The cryoballoon catheter is introduced into the left atrium. The physician inflates the balloon and moves it to the opening of the pulmonary vein. The goal is to close off the opening of the pulmonary vein completely, which stops the flow of blood between the atrium and the vein (this is called occlusion). Once occlusion is confirmed, the physician introduces liquid refrigerant into the balloon. The refrigerant evaporates and removes heat from the heart tissue at the opening of the pulmonary vein where the balloon is in contact with it. As a result, the tissue is scarred and may no longer spread the electrical currents that cause atrial fibrillation.
HOW ARCTIC FRONT ADVANCE CRYOBALLOON WORKS
Arctic Front Advance cryoballoon creates circumferential lesions, isolating each pulmonary vein with minimal energy applications, delivering consistent and repeatable results. Arctic Front Advance provides physicians a straightforward four-step approach for PVI.
STRAIGHTFORWARD 4-STEP PROCEDURE
Step 1: Access Targeted Vein
The cryoballoon is deployed in the left atrium and the Achieve™ Mapping Catheter is inserted into the target vein.

Step 2: Inflate and Position
The cryoballoon is inflated in the atrium before being advanced toward the wired vein. The balloon is then positioned at the antrum of the pulmonary vein.
Step 3: Complete Occlusion
Contrast dye is then injected through the guide-wire lumen to assess vein occlusion via fluoroscopy.

Step 4: Ablate and Assess PVI
The cryoballoon ablates where the balloon is in contact with the tissue. The device’s anatomical shape and large surface area creates circumferential lesions with minimal energy applications. The Achieve Mapping Catheter is then used to confirm pulmonary vein isolation.

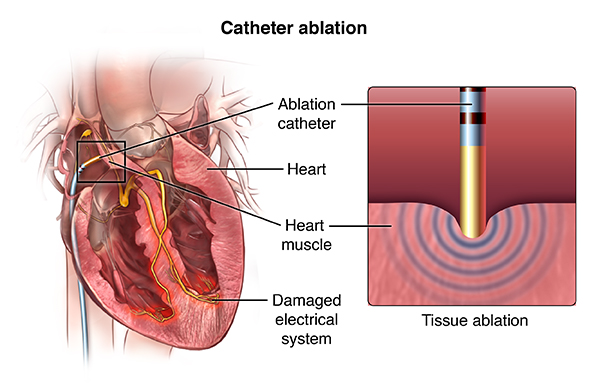
Radiofrequency Catheter Ablation of Arrhythmias
This technique has proved curative for many different types of arrhythmias. In the late 1980’s, during his electrophysiology fellowship at Yale, Dr. Marieb visited Dr. Warren (Sonny) Jackman in Oklahoma City. Dr. Jackman is considered the pioneer in the field of radiofrequency catheter ablation, and initially began using the procedure for supraventricular tachycardia (SVT) due to AV nodal reentrant tachycardia and SVT due to accessory pathways. After visiting Dr. Jackman twice, Dr. Marieb brought his training experience back to Yale, where he began performing the procedure almost 30 years ago. Since that time the use of this procedure has expanded dramatically.
Dr. Marieb performs this procedure for many different types of arrhythmias. This includes supraventricular tachycardia due to AV nodal reentrant tachycardia, atrial tachycardia, and SVT due to accessory pathways including the Wolf Parkinson White syndrome. Other arrhythmias that are routinely treated with this procedure include ablation of atrial fibrillation, atrial flutter, ventricular tachycardia, and frequent premature ventricular contractions, as well as catheter ablation of the atrioventricular node. Cryoablation is also performed for arrhythmias originating near the AV node in normal electrical system of the heart. This helps avoid the risk of injury to the natural electrical connections of the heart, avoiding pacemaker implantation. We also offercryo-balloon ablation for paroxysmal atrial fibrillation.
The procedure is typically performed under sedation either with intravenous sedation or even general anesthesia. The femoral veins are typically used to access the heart; sometimes the femoral arteries are used. Thus this is not technically a surgical procedure although invasive. The procedure can take anywhere between two and eight hours. Electro-anatomical mapping systems are used to help guide the ablation and reduce x-ray and fluoroscopic exposure. Initially the arrhythmias are “mapped”; once localized the ablation catheter is navigated to the area of interest and radio frequency energy is delivered through the tip of the catheter which essentially heats and destroys the tissue responsible for the arrhythmia. The success rates are high. However, they do vary in regards to patient characteristics as well as the type of arrhythmia itself. For instance, ablation of atrial fibrillation carries a lower success rate than other types of arrhythmias. It should be noted that there are some risks of the procedure as it is invasive. These include and are not limited to heart block requiring a pacemaker, stroke, death, hole in the heart requiring drainage of blood from around the heart or surgery, damage to heart valve or vessels, bleeding, vessel injury where the catheters are inserted, phrenic nerve damage interfering with diaphragmatic function and breathing, among other more rare complications. Overall, these complications are not very common, but need to be considered in decision-making.
In most cases, the patient is discharged on the following day and can return to work within a few days. There are some patients who will experience a recurrence of their arrhythmia, but most are permanently cured. If there is a recurrence the success rate of a repeat procedure is high.
Contact Force Sensing Ablation Catheter
This catheter enables direct and real-time measurement of contact force during radiofrequency catheter ablation procedures for patients suffering from drug-resistant paroxysmal atrial fibrillation (Afib), sustained monomorphic ischemic ventricular tachycardia (VT) and Type I atrial flutter. Biosense Webster Inc.’s Thermocool Smarttouch Catheter provides continuous contact force information when applying radiofrequency energy (RF) against the heart wall. This information has been shown to improve outcomes; inconsistent tissue contact may result in incomplete lesion formation that could result in inefficacy and the need for additional treatment, and too much contact may result in tissue injury, which may lead to complications, including perforation of the heart. The Thermocool Smarttouch Catheter provides direct, real-time quantitative feedback graphically displayed on the company’s Carto 3 System upon tissue contact.

The Thermocool Smarttouch Catheter was evaluated as part of a prospective, multicenter study called the SMART-AF Trial in patients with drug-resistant symptomatic paroxysmal atrial fibrillation. One-year results from the trial showed that patients experienced a 74 percent overall success rate after treatment with the Thermocool Smarttouch Catheter. Data from the trial showed higher success rates the longer physicians stayed within a targeted contact force range, with one-year results demonstrating an 88 percent success rate when physicians stayed within a targeted range greater than or equal to 85 percent of the time. The trial demonstrated for the first time that it is the consistent and stable application of contact force on the heart wall that positively impacts the efficacy of the procedure in this patient population.
HIS Bundle Pacing
This newer pacing technology involves placing a pacing lead at the area of the HIS bundle, or bundle of HIS. This electricalbundle is part of the natural electrical conduction system of the heart, branching into the Right bundle branch and Left bundle branch, which rapidly transmit electrical signals to the Right and Left ventricles. The advantage of pacing the bundle of HIS is that the electrical signals then travel over the normal pathways of the natural electrical system, rapidly reaching the two ventricles simultaneously, avoiding dyssynchrony (electrical delay between the 2 ventricles, which can cause inefficient contraction of the ventricles and even weakening of the heart muscle). The technique can be a bit challenging, as it involves screwing a pacing lead into a very specific area, and is not always successful. However, when it is successful, pacing this area can closely mimic normal electrical activity and overcome the disadvantages of pacing the ventricles in areas far away from the natural electrical system.

Rhythmia HDX Mapping System
Boston Scientific Corporation’s RHYTHMIA HDx Mapping System sets a new bar in high-definition mapping by using three main features that sets it apart from older mapping systems: density (high density 64 electrodes used to acquire data), resolution (signals too small to be detected by other systems are able to be recorded and evaluated), and automation (computer algorithms are used to interpret signals and discard signals that are not physiologically relevant). The system can be used to map and figure out very complex electrical circuits in the heart, which leads to more accurate and effective ablation. The catheter used to acquire these signals is called the Orion catheter, and is displayed below. An example of maps created by this innovative system are displayed below.

DV-8 Esophageal Retractor System and Circa-S Temperature Probe
One of the most feared complications of ablation of atrial fibrillation is an atrio-esophageal fistula. This complication occurs when a connection forms between the esophagus and atrium; it typically occurs 2-4 weeks after the ablation procedure. Unfortunately, if the complication occurs, it is often fatal, as air and bacteria enter the left atrium from the esophagus.
The complication likely occurs due to injury to the esophagus from ablation of the posterior portion of the left atrium, which is often an important area to ablate. The esophagus typically is in close proximity to at least a portion of the posterior wall of the left atrium.
In order to try to prevent this complication, we often use a highly accurate temperature probe in the esophagus to detect heating during the procedure. The Circa-S probe has multiple temperature sensors that span a wide area of the esophagus. In addition, these sensors respond very rapidly to rises in temperature, and alert the operator to esophageal heating which theoretically can signal esophageal injury.
Possibly more importantly, as the esophagus often lies directly over areas that may be important to achieve a successful ablation, we are now often using the DV-8 esophageal retractor system to move or deviate the esophagus away from the area of ablation. Theoretically this might decrease the chance of esophageal injury and allow ablation of areas that may be important to the success of the ablation procedure.

Circa S multielectrode esophageal temperature probe



Use of the Circa-S esophageal temperature probe and the DV-8 esophageal retractor together